

Radiology in 2015

In the spirit of the New Year, we checked out Diagnostic Imaging's predictions for 2015. We thought their guesses were quite spot on, check them out below:
Lung Cancer Low Dose CT
- Resolution of details of LDCT coverage between CMS and payers, for example upper end of age limit (CMS says 74, USPSTF says 80).
- ACR will work to ensure implementation of a high quality LDCT program and that service is reimbursed at a level that will optimize access for patients
Imaging 3.0
- Continue to guide radiologists through a time of transition in health care and inform patients, other health care providers, payers and policy makers about the value that radiologists deliver
- More non-radiology stakeholders (patients, hospital administrators, health systems) will expect radiologists to provide non-interpretive services
Decision Support
- The Medicare Demonstration project yielded fairly tepid support for the notion that decision support help referring clinicians order more appropriate imaging procedures, with the 2017 start date for required radiology order entry decision support, 2015-2016 may produce some new studies to measure the impact
- The ascendancy of imaging informatics: A big part of radiology’s foreseeable future will be about software, not hardware. Across the board – business analytics, visualization, reporting, decision support, imaging sharing – informatics will be key to achieving value, improving quality and advancing our patients’ interests.
Reimbursement:
- Continued cuts in radiology reimbursement, but rate of change will slow in the short term. Practices should use that relative reprieve as an opportunity to focus on how they will be compensated under emerging payment models.
- Declining reimbursement will result in an inappropriate emphasis on productivity, more significant turf battles, and a growing tendency to commoditize the specialty.
- Radiology advocacy will play an extremely important role in combating harsh cuts to reimbursement.
Dose:
- Decreased interest in dose reduction. The topic, which has been popular for the last several years, may have run its course. Radiologists are more interested in diagnostic quality rather than dose reduction.
- Radiologists will push for 3D mammography and dual energy CT techniques, despite the larger radiation doses.
Training and Jobs:
- The first crop of board-eligible radiology fellows will venture into the working world. It will be interesting to see how the new graduates, payors and practices adapt to the change, whether new hires will be given adequate time to prepare for the second part of their examination and how practices will adapt if the new hire doesn’t pass the exam.
- Anecdotally, it seems that the job market is picking up. This provides an opportunity for those who accepted less-than-ideal jobs to seek new employment. Because these hires will already be board-certified, it will be interesting to see if there is a lot of turnover of this particular group.
- The number of applicants for radiology residency is down again this year, which may mean that programs need to start considering cutting down on their class sizes.
Seen here: What Will Radiology Look Like in 2015?
What Are Healthcare Practices Thankful For?
This week marks the kickoff of the season of giving. On Thursday, we’ll be celebrating the season of giving THANKS, thanks for our loved ones, whoever invented deep fried turkey, the NFL network and four-day weekends with our friends and family. Thinking about what we are thankful for in our personal lives got us thinking about what we are thankful for at our practices across the country and we realized that there so, so many. Hopefully as you read through our list you’ll realize how thankful you are for the same things at your practice. Maybe you’ll even add some of your own to the list in our comment section!
1. Our practices wouldn’t be anything without our patients, so as always they are our #1. We know they can go anywhere for their care, so when they choose us, it’s an honor.
2. We are thankful for our referring physician offices that entrust their patients’ care to our hands. We value your trust and are proud to work as an extension of your practice.
3. Our staff members are dedicated, coming in early or staying late, just so we can fit a patient into the schedule during a time that works for them. They don’t complain about coming in after hours, because they know it will help the practice in the long run.
4. It’s funny to think of your equipment vendors as a part of your practice, but sometimes we require their support and we are thankful that they are able to be there for us when we need them.

5. We are thankful for the owners of our independent centers. In our industry there is a lot of pressure to get bought out by hospital systems due to decreasing reimbursement, but our centers’ owners understand the value of remaining independent and have chosen to take the path less traveled.
6. The life of a marketing representative can be flat out exhausting. They are constantly on the road, out in the community showing what is so great about our centers. Additionally, they are always looking for ways to help make their referring offices’ staff happy, which means they are always bending over backwards to help.
7. We’re thankful for Yelp because it helps us gather reviews for our centers. It allows patients to hear from other patients about their positive experiences at our centers. On the flip side, if a patient doesn’t have a perfect experience for any reason, it gives them a way to let us know so that we can fix it.
8. Salesforce is our marketing savior on a daily basis. The CRM helps us track referring offices, keep track of meetings and grow our centers’ success, so we’re pretty thankful that we have access to this awesome platform.
9. We’re extra thankful for our office Keurigs. Because coffee. Coffee. Coffee. Coffee. Need we say more?
10. Lastly, we are thankful for Jean Fridays! We are lucky enough to basically wear pajamas (read: scrubs) every day, but there is just something about getting to wear jeans on Friday that screams “WEEKEND!”
Tell us what your practice is thankful for this Thanksgiving…
RBMA Hot Topic: ICD-10 Implementation Perception

RBMA’s Hot Topic Question of the week relates to the impending implementation of ICD-10. For the last year the date of implementation has continued to be pushed back, leaving providers unsure when it will really go into effect. Most providers seem to be pleased by it’s delay because it means they don’t have to learn the new coding system, but it is only a matter of time before we all will need to adapt to the ICD-10 protocols.
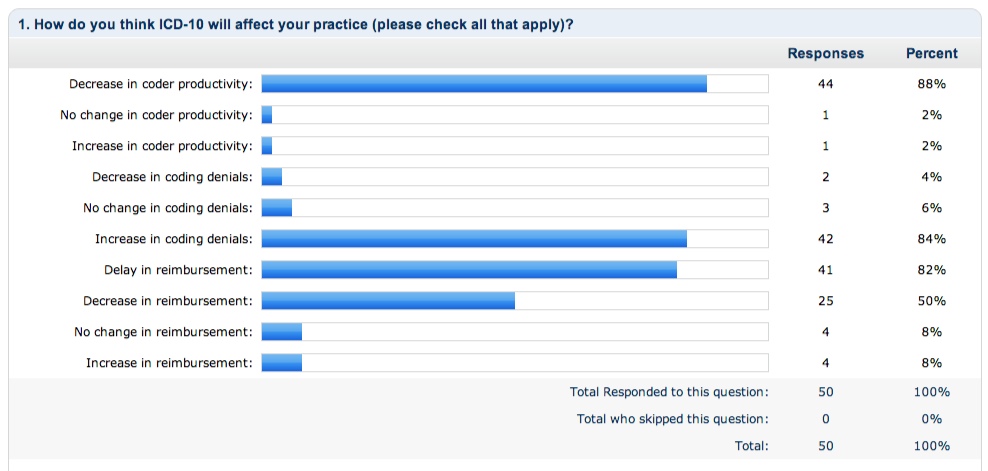
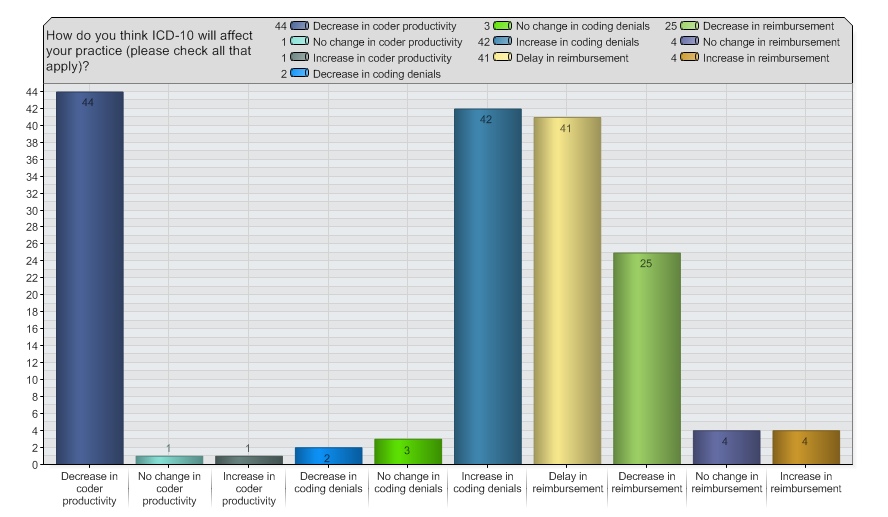
The RBMA took to the forums to find out for real how health care professionals in radiology feel about ICD-10 and how it will affect their practice. The survey is still running, but the largely negative response is overwhelming. Participants were asked, “How do you think ICD-10 will affect your practice? Check all that apply.” Options included:
- Decrease in coder productivity
- No change in coder productivity
- Increase in coder productivity
- Decrease in coding denials
- No change in coding denials
- Increase in coding Denials
- Delay in reimbursement
- Decrease in reimbursement
- No change in reimbursement
- Increase in reimbursement
Participate in the survey > Click Here
Currently, the most popular responses reflect the belief that implementation will bring decreased coder productivity, increased coding denials, delayed reimbursement and decreased reimbursement overall.
So, what’s with the all this ICD-10 hating? First of all, there are SO many changes with the new codes. (Review them all here: ICD-10 Education) It is intimidating, especially for those who are already not experts with ICD-9 coding. Many practices and organizations have kept their revenue cycle management in-house for so long, in an effort to cut costs and keep control, but that trend will come to an end.
In theory, ICD-10 should help physicians improve their reimbursements and cut down denials, however that is only if the codes are used appropriately. Heed the warning signs and start preparing now, because ready or not… ICD-10 is coming.
Building Better Marketing Programs: RBMA Wrap-Up
The RBMA Building Better Marketing Conference in Long Beach, California went off without a hitch earlier this week, bringing together the best radiology professionals from all across the world. On Sunday evening, the attendees mingled in the lobby of the Renaissance Long Beach hotel meeting new friends and reminiscing with the old. With the sound of an acoustic guitar in the background and the sea breeze filtering through the open doors, everyone knew we had arrived in Cali baby.
Monday morning is hard for everyone, but Terri Langhans opening presentation got everyone’s gears going for the week. She asked us, “How do you stand out in an industry where everyone looks alike?” By comparing the radiology industry to the airline industry she led us to see the opportunities available to make ourselves stand out. Think about the differences in flying Southwest versus Delta, even just the comedic way Southwest delivers their safety information. “You don’t have to be a comedian, you just have to have a personality,” Langhans quoted. Her message was to make sure we do small things with character, because the more similar you are, the more your differences matter.
In radiology, each touch point your patients have with your center matters. A touch point is any point of contact, for instance; phone trees, parking, welcomers, front desk employees, techs, radiologists, schedulers, even your billing department. Langhans’ message essentially, is that your touch points should be talking points, or components that set you apart from the competition and contribute to a strong culture for your organization.
(Check out photos from the event on the RBMA Facebook Page here: https://www.facebook.com/RBMAConnect)
The schedule over the next two days was packed full of sessions covering content including:
- Writing creative marketing/web content
- Social media for radiology providers
- Stark Law and Sunshine Act
- Advancements in breast imaging
- Search engine optimization
- Selecting and utilizing a CRM
- Rebranding techniques
- Using referral metrics to drive business
- Finding an “Open Table” model for radiology scheduling
- Interventional radiology practice development
- Imaging market changes and opportunities
- Content marketing strategies
- Customer service and efficiency
- Campaign creation versus ads
- Benchmarking for marketing and sales
- Quality initiatives for independent hospital-based physicians
- Advice for IDTFs competing with hospital systems
In addition to those very focused sessions, conference attendees gathered together for roundtables discussing marketing efforts they have used that were effective and the industry issues that have been keeping them up at night. Tuesday morning was also kicked off by a 5 Minute Forecast from a panel of RBMA experts. All of whom were geniuses; well spoken and wonderful. (Cough, cough… this is shameless brag, as I was one of them.) After the forecasts, which predicted increases in patient-consumerism, market transparency and the increased weight of strong industry relationships, the floor was opened up to the attendees and they were given the chance to ask any marketing questions they had up their sleeves. The session, entitled “Stump The Marketers,” was my favorite part of the entire conference because it enabled us to engage in candid conversation about the real issues we all face on a daily basis. Topics covered included:
- ICD-10 and the effect on marketing representatives: It was determined that the coding changes will give marketers a chance to stand out as early adopters and even give training opportunities to their referring offices.
- Direct targeting and re-targeting campaigns for patients: Some wondered if this form of internet marketing could be considered invasive, but we decided that if the patient is already interested in you, they will perceive you in that way.
- Utilizing technology for patient communication: We decided that nothing can be replaced by one-on-one communication and people do not want to be made more convenient. If a patient ops in for email or text reminders or event updates, that is another opportunity.
- Spending money on traditional marketing and advertising like the phonebook: These historically expensive methods have no way of being measured as far as ROI goes, so most marketing pros have started to turn towards internet marketing instead.
Anyone that was a part of the conference will say that they learned a lot and will remember fondly how great the smartphone application was (especially with the neck-in-neck race between Erik W. and Brenda B. for top users), the great bartenders at "Sip", the great elevator struggle of 2014, the California-themed Quest Awards and how wonderful the RBMA faculty was for organizing such a spectacular event.
Overall the conference was a huge success. The RBMA team certainly knows what they are doing and each year the content and sessions get better and better. We are already looking forward to next year’s event, it is going to be in Nawlins’ after all! Until next year everyone, can’t wait to see what all we will accomplish in 2014.